Common Procedures

Regular Exams and Cleanings
Regular exams are an important part of maintaining your oral health. During your regular exam, we will:
- Check for any problems that you may not see or feel
- Look for cavities or any other signs of tooth decay
- Inspect your teeth and gums for gingivitis and signs of periodontal disease
- Provide a thorough teeth cleaning
- Oral hygiene instruction
- Diet and nutrition counselling
- Orthodontic screening
Your regular exam will take about 30 minutes. Each regular exam includes a detailed teeth cleaning, in which we will clean, polish, and rinse your teeth to remove any tartar and plaque that has built up on the tooth's surface.
Visiting our office every six months gives you the chance to talk the doctor about any questions you may have about your oral health. Regular exams are offered by appointment only, so please contact our practice today to schedule your next dental exam and teeth cleaning.
Crowns
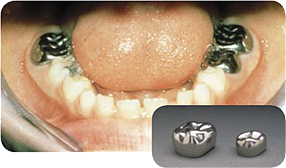 Crowns are a cosmetic restoration used to improve the tooth’s shape or to strengthen a tooth. Crowns are most often used for teeth that are broken, worn, or have portions destroyed by tooth decay.
Crowns are a cosmetic restoration used to improve the tooth’s shape or to strengthen a tooth. Crowns are most often used for teeth that are broken, worn, or have portions destroyed by tooth decay.
A crown is a "cap" cemented onto an existing tooth that fully covers the portion of the tooth above the gum line. In effect, the crown becomes the tooth’s new outer surface.
Stainless steel crowns have proven to be a very successful restoration for large cavities on primary teeth. They'll last as long as the remaining primary tooth would have lasted, and their failure rate is very low.
Digital X-Rays
 Radiographs (X-Rays) are a vital and necessary part of your child's dental diagnostic process. Without them, certain dental conditions can and will be missed.
Radiographs (X-Rays) are a vital and necessary part of your child's dental diagnostic process. Without them, certain dental conditions can and will be missed.
Radiographs detect much more than cavities. For example, radiographs may be needed to survey erupting teeth, diagnose missing or supernumerary (extra) teeth, diagnose bone diseases, evaluate the results of an injury, or plan orthodontic treatment. Radiographs allow dentists to diagnose and treat health conditions that cannot be detected during a clinical examination. If dental problems are found and treated early, dental care is more comfortable for your child and more affordable for you.
The American Academy of Pediatric Dentistry recommends radiographs and examinations every six months for children with a high risk of tooth decay. On average, most pediatric dentists request radiographs approximately once a year. Dr. Trimboli and Dr. Brown use a risk-assessment approach to prescribing radiographs, as recommended by the AAPD. Patients who are at low risk for decay may only need x-rays once every 1.5 years. Approximately every 3 years, it is a good idea to obtain a complete set of radiographs, either a panoramic film and bitewings or periapical films and bitewings.
Pediatric dentists are particularly careful to minimize the exposure of their patients to radiation. With contemporary safeguards, the amount of radiation received in a dental X-ray examination is extremely small. The risk is negligible. In fact, the dental radiographs represent a far smaller risk than an undetected and untreated dental problem. Lead body aprons and shields will protect your child. Today's equipment filters out unnecessary x-rays and restricts the x-ray beam to the area of interest. High-speed film and proper shielding assure that your child receives a minimal amount of radiation exposure.
Extractions
 There are times when it is necessary to remove a tooth. Sometimes a baby tooth has misshapen or long roots that prevent it from falling out as it should, and the tooth must be removed to make way for the permanent tooth to erupt. At other times, a tooth may have so much decay that it puts the surrounding teeth and jaw at risk of decay, so your doctor may recommend removal and replacement with a bridge or implant. Infection, orthodontic correction, or problems with a wisdom tooth can also require removal of a tooth.
There are times when it is necessary to remove a tooth. Sometimes a baby tooth has misshapen or long roots that prevent it from falling out as it should, and the tooth must be removed to make way for the permanent tooth to erupt. At other times, a tooth may have so much decay that it puts the surrounding teeth and jaw at risk of decay, so your doctor may recommend removal and replacement with a bridge or implant. Infection, orthodontic correction, or problems with a wisdom tooth can also require removal of a tooth.
When it is determined that a tooth needs to be removed, your dentist may extract the tooth during a regular checkup or may request another visit for this procedure. The root of each tooth is encased within your jawbone in a "tooth socket," and your tooth is held in that socket by a ligament. In order to extract a tooth, your dentist must expand the socket and separate the tooth from the ligament holding it in place. While this procedure is typically very quick, it is important to share with your doctor any concerns or preferences for sedation.
Once a tooth has been removed, neighboring teeth may shift, causing problems with chewing or with your jaw joint function. To avoid these complications, your dentist may recommend that you replace the extracted tooth.
Fillings
 Traditional dental restoratives, or fillings, may include gold, porcelain, and composite. The strength and durability of traditional dental materials continue to make them useful for situations where restored teeth must withstand extreme forces that result from chewing, such as in the back of the mouth.
Traditional dental restoratives, or fillings, may include gold, porcelain, and composite. The strength and durability of traditional dental materials continue to make them useful for situations where restored teeth must withstand extreme forces that result from chewing, such as in the back of the mouth.
Newer dental fillings include ceramic and plastic compounds that mimic the appearance of natural teeth. These compounds, often called composite resins, are usually used on the front teeth where a natural appearance is important, as well as on the back teeth depending on the location and extent of the tooth decay.
What's Right for Your Child?
Several factors influence the performance, durability, longevity and expense of dental restorations, including:
- The components used in the filling material
- The amount of tooth structure remaining
- Where and how the filling is placed
- The chewing load that the tooth will have to bear
- The length and number of visits needed to prepare and adjust the restored tooth.
Before your child's treatment begins, the doctor will discuss with you all of your options, and help you choose the best filling for your child's particular case. To help you prepare for this discussion it may be helpful to understand the two basic types of dental fillings — direct and indirect.
- Direct fillings are placed immediately into a prepared cavity in a single visit. They include glass ionomers, resin ionomers, and composite (resin) fillings. The dentist prepares the tooth, places the filling, and adjusts it in just one appointment.
- Indirect fillings generally require two or more visits. They include inlays, onlays, veneers, crowns, and bridges fabricated with gold, base metal alloys, ceramics, or composites. During the first visit, the dentist prepares the tooth and makes an impression of the area to be restored. The dentist then places a temporary covering over the prepared tooth. The impression is sent to a dental laboratory which creates the dental restoration. At the next appointment, the dentist cements the restoration into the prepared cavity and adjusts it as needed.
Fluoride
Fluoride is an element that has been shown to be beneficial to teeth. However, too little or too much fluoride can be detrimental to the teeth. Little or no fluoride will not strengthen the teeth to help them resist cavities. Excessive fluoride ingestion by preschool-aged children can lead to dental fluorosis, which is a chalky white to even brown discoloration of the permanent teeth. Many children often get more fluoride than their parents realize. Being aware of a child's potential sources of fluoride can help parents prevent the possibility of dental fluorosis.
Some of these sources are:
- Too much fluoridated toothpaste at an early age.
- The inappropriate use of fluoride supplements.
- Hidden sources of fluoride in the child's diet.
The use of fluoride has been found to be a major factor in the reduction of dental caries. When used appropriately, fluoride is both safe and effective. Fluoride is found in many different sources and frequent exposure to small amounts each day will best reduce the risk of dental caries. Drinking fluoridated water and using a toothpaste containing fluoride to brush with at least twice a day goes a long way in preventing dental decay. If you are uncertain whether you are in a fluoridated water community call your local water utilities to be sure. Other sources of fluoride, such as fluoride drops, tablets, and rinses should only be used on the advice of your dentist, to insure that you are not getting too little or too much fluoride. However, for those patients that present with a high caries rate your pediatric dentist my recommend toothpaste that contain higher levels of fluoride and rinses to help reduce decay.
Two and three year olds may not be able to expectorate (spit out) fluoride-containing toothpaste when brushing. As a result, these youngsters may ingest an excessive amount of fluoride during toothbrushing. Toothpaste ingestion during this critical period of permanent tooth development is the greatest risk factor in the development of fluorosis.
Excessive and inappropriate intake of fluoride supplements may also contribute to fluorosis. Fluoride drops and tablets, as well as fluoride-fortified vitamins should not be given to infants younger than six months of age. After that time, fluoride supplements should only be given to children after all of the sources of ingested fluoride have been accounted for and upon the recommendation of your pediatrician or pediatric dentist.
Certain foods contain high levels of fluoride, especially powdered concentrate infant formula, soy-based infant formula, infant dry cereals, creamed spinach, and infant chicken products. Please read the label or contact the manufacturer. Some beverages also contain high levels of fluoride, especially decaffeinated teas, white grape juices, and juice drinks manufactured in fluoridated cities.
Parents can take the following steps to decrease the risk of fluorosis in their children's teeth:
- Use baby tooth cleanser on the toothbrush of the very young child.
- Place only a pea-sized drop of children's toothpaste on the brush when brushing.
- Account for all of the sources of ingested fluoride before requesting fluoride supplements from your child's physician or pediatric dentist.
- Avoid giving any fluoride-containing supplements to infants until they are at least 6 months old.
- Obtain fluoride level test results for your drinking water before giving fluoride supplements to your child (check with local water utilities).
Mouthguards
 When a child begins to participate in recreational activities and organized sports, injuries can occur. A properly fitted mouth guard, or mouth protector, is an important piece of athletic gear that can help protect your child's smile, and should be used during any activity that could result in a blow to the face or mouth. Mouth guards help prevent broken teeth, and injuries to the lips, tongue, face or jaw. A properly fitted mouth guard will stay in place while your child is wearing it, making it easy for them to talk and breathe.
When a child begins to participate in recreational activities and organized sports, injuries can occur. A properly fitted mouth guard, or mouth protector, is an important piece of athletic gear that can help protect your child's smile, and should be used during any activity that could result in a blow to the face or mouth. Mouth guards help prevent broken teeth, and injuries to the lips, tongue, face or jaw. A properly fitted mouth guard will stay in place while your child is wearing it, making it easy for them to talk and breathe.
A custom mouth guard has the most superior fit and comfort level. An impression is taken in the dental office and a guard is made to fit the mold. They come in a variety of colors and are perfect for those that have completed orthodontic treatment and have all permanent teeth.
Another alternative is a customized boil-and-bite mouth guard that may be purchased at a sports store or pharmacy. The guard is dipped in boiled water for 30 seconds and then placed in the mouth, the patient bites for a customized fit. Although the fit is not as good as the customized guard it is good for those patients that have teeth coming in and out and may need more then one guard during the season. Stock mouth guards are one size fits all. They have the least amount of retention and fit but are far better than wearing nothing at all.
Ask your pediatric dentist about custom and store-bought mouth protectors.
Types of mouthguards
Choosing the right mouthguard is essential. There are three basic types of mouthguards: the pre-made mouthguard, the "boil-and-bite" fitted mouthguard, and a custom-made mouthguard from your dentist. When choosing a mouthguard, be sure to pick one that is tear-resistant, comfortable and well fitted for your child's mouth, easy to keep clean, and does not prevent him from breathing properly. If he wears braces or a retainer, it is imperative for him to wear a mouthguard. Your dentist can show your child how to wear a mouthguard properly and how to choose the right mouthguard to protect his smile.
Taking care of your mouthguard
Similar to a retainer, braces, or any other special dental appliance, it is important to take care of your child's mouthguard by storing it properly and keeping it clean, as well as knowing when to replace an old mouthguard with a new one. Here are a few simple ways to keep your child's mouthguard clean and working correctly:
- Gently scrub the mouthguard after each use with a toothbrush and toothpaste.
- Store the mouthguard in a protective case.
- Do not leave the mouthguard in the sun or in hot water, as it may melt or become deformed.
- Replace the mouthguard at the beginning of every new sports season. You should also replace your child's mouthguard if you notice it has become worn and not longer fits properly.
- Do not wear a retainer with a mouthguard. If your child wears braces, your dentist will help design a mouthguard to protect his teeth and his braces.
- Do no chew on or cut pieces off of your mouthguard. Mouthguards come in different shapes and sizes, so ask your dentist which is best for your child.
- Bring the mouthguard to each dental checkup and the dentist can check to make sure it's still in good shape!
Sealants
 Sometimes brushing is not enough, especially when it comes to those hard-to-reach spots in your child's mouth. It is difficult for a toothbrush to get in between the small cracks and grooves on teeth. If left alone, those tiny areas can develop tooth decay. Sealants give your child's teeth extra protection against decay and help prevent cavities.
Sometimes brushing is not enough, especially when it comes to those hard-to-reach spots in your child's mouth. It is difficult for a toothbrush to get in between the small cracks and grooves on teeth. If left alone, those tiny areas can develop tooth decay. Sealants give your child's teeth extra protection against decay and help prevent cavities.
Dental sealants are a plastic resin that bonds and hardens in the deep grooves on the tooth's surface. When a tooth is sealed, the tiny grooves become smooth, and are less likely to harbor plaque. With sealants, brushing becomes easier and more effective against tooth decay.
Sealants are typically applied to children's teeth as a preventive measure after the permanent teeth have erupted as a way to prevent tooth decay. It is more common to seal "permanent" teeth rather than "baby" teeth, but every patient has unique needs, and the dentist will recommend sealants on a case-by-case basis.
Sealants last from three to five years, although it is fairly common to see adults with sealants still intact from their childhood. A dental sealant only provides protection when it is fully intact so if your child's sealants come off, let the dentist know, and schedule an appointment for your child's teeth to be re-sealed.
Space Maintainers
 Sometimes a primary tooth is lost before the permanent tooth beneath it is ready to erupt. The most common causes for this are cavities and injuries. If your child loses a tooth prematurely we may recommend a space maintainer. A space maintainer is an appliance that holds open the space left by the lost tooth.The space maintainer helps prevent the nearby teeth from shifting into the vacant space. If this happens, when the permanent tooth is ready to erupt may not have enough room or may erupt in a wrong position.Once the spacer is in place, the eruption of the permanent tooth is monitored and when the time is right, the spacer is removed.
Sometimes a primary tooth is lost before the permanent tooth beneath it is ready to erupt. The most common causes for this are cavities and injuries. If your child loses a tooth prematurely we may recommend a space maintainer. A space maintainer is an appliance that holds open the space left by the lost tooth.The space maintainer helps prevent the nearby teeth from shifting into the vacant space. If this happens, when the permanent tooth is ready to erupt may not have enough room or may erupt in a wrong position.Once the spacer is in place, the eruption of the permanent tooth is monitored and when the time is right, the spacer is removed.
Wisdom Teeth
 Wisdom teeth are molars found in the very back of your mouth. These teeth usually appear in late teens or early twenties but may become impacted (fail to erupt) due to lack of room in the jaw or angle of entry. When a wisdom tooth is impacted, it may need to be removed. If it is not removed, you may develop gum tenderness, swelling, or even severe pain. Impacted wisdom teeth that are partially or fully erupted tend to be quite difficult to clean and are susceptible to tooth decay, recurring infections, and even gum disease.
Wisdom teeth are molars found in the very back of your mouth. These teeth usually appear in late teens or early twenties but may become impacted (fail to erupt) due to lack of room in the jaw or angle of entry. When a wisdom tooth is impacted, it may need to be removed. If it is not removed, you may develop gum tenderness, swelling, or even severe pain. Impacted wisdom teeth that are partially or fully erupted tend to be quite difficult to clean and are susceptible to tooth decay, recurring infections, and even gum disease.
Wisdom teeth are typically removed in the late teens or early twenties because there is a greater chance that the teeth's roots have not fully formed and the bone surrounding the teeth is less dense. These two factors can make extraction easier, as well as making the recovery time much shorter.
In order to remove a wisdom tooth, your dentist first needs to numb the area around the tooth with a local anesthetic. Since the impacted tooth may still be under the gums and imbedded in your jaw bone, your dentist will need to remove a portion of the covering bone to extract the tooth. In order to minimize the amount of bone that is removed with the tooth, your dentist will often "section" your wisdom tooth so that each piece can be removed through a small opening in the bone. Once your wisdom teeth have been extracted, the healing process begins. Healing time varies depending on the degree of difficulty related to the extraction. Your dentist will share with you what to expect and provide instructions for a comfortable, efficient healing process.
Common Procedures
/ Invisalign
/ Teeth Whitening
/ Opalescence